
The Problem with Prozac
The Problem with Prozac
Why seeking happiness never really gets us anywhere

“Happiness cannot be pursued; it must ensue.”
Viktor E. Frankl, Man's Search for Meaning
At this point, the rest of this post is superfluous. Frankl’s quote is just that good. Or at least that’s how I feel about it. A brief aside before starting our journey: quotes really come alive when you know the context. I often find it amazing how one quote really speaks to one person but is nothing more than a pithy placard to the next. Hopefully the quote above isn’t that to those reading. But if it is, then I strongly recommend reading Man’s Search for Meaning - Frankl’s autobiographical account and observations, as a psychiatrist, in the Nazi concentration camps during World War II.
This ties into the main feature: that we don’t understand happiness (or other emotions for that matter), and that fulfillment, finding meaning, gets put on the backburner. While this isn’t necessarily the main thrust of Man’s Search for Meaning, it is a core theme - so much so that Frankl developed a new kind of therapy called logotherapy, focused on patients finding meaning, after his experience in the camps. Frankl shares about how Holocaust inmates who had a purpose seemed to survive longer than those who didn’t, regardless of food or living conditions. He spends the later part of the book talking about his thoughts. Central in these thoughts, he frames negative emotions in a healthier light. He describes feeling hopeless, sad, or stressed as important emotions in their own right, and he highlights that avoiding these emotions (which often happens when we characterize them negatively) leads to negative outcomes.
Let’s bring this back to Prozac, to the diagnosing of mental illness and the prescribing of psychotropic medications. It is important to know that depression, clinically called major depressive disorder, is only a group of symptoms. There is no clear root cause of depression; better said: we don’t know the root cause of depression, or depression may actually be many different disorders all with their own causes. Some people may be depressed because they have hormone deficiencies, others may have certain genes that are activated or inactive, still others may have depression because of excessive inflammation or an imbalanced gut microbiome. We really have no idea. Most people working in psychiatry know this. Most people in the general public do not. Unfortunately, I believe it is Moloch, the hubris of medical professionals and the greed of pharmaceutical companies, that prevents the spreading of this knowledge.
Now, what does this mean? It doesn’t mean that we don’t have treatments that help depression. It doesn’t mean that depression doesn’t exist or that people don’t experience depression. It means that we don’t know much; we have a lot to learn. It means that a diagnosis of depression today is nothing more than a checklist of symptoms like this:
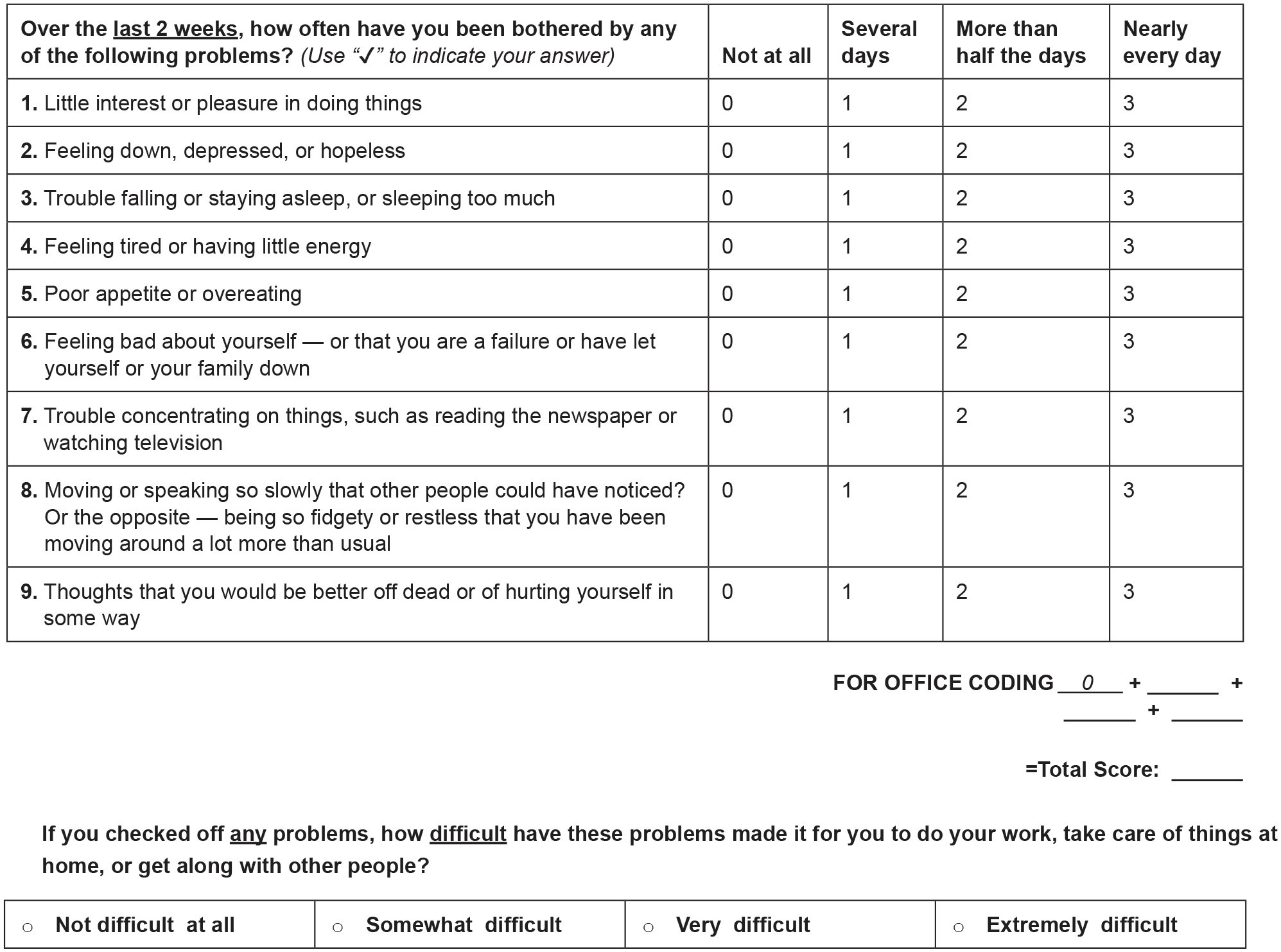
Again, I want to emphasize that there is still a benefit to figuring out if someone has major depressive disorder. It helps us know what treatments to use. But all we are doing is trying to reduce symptoms that fall under the umbrella of depression.
Where am I going with all of this? Well, the question becomes how severe should depression be before we use medication to treat it? This is a very hard question and different patients and providers will give vastly different answers. But the most common answer is whenever a patient comes in for help and says they are depressed. There are almost no occurrences of patients coming in for treatment of depression and the provider turning them away because the provider doesn’t think they are depressed enough for treatment. Hell, even primary care providers don’t hold back antibiotics nearly as often as they should; they fold to the pressure of patients. Patients (people like you and I) are constantly asking doctors and nurse practitioners for inappropriate requests: medically unnecessary labs, antibiotics to treat viruses, or imaging like MRIs when the chance of benefit is miniscule. I would venture to place antidepressant and anti-anxiety medication in this category as well. They all have appropriate use cases, but in America, we like our medicine.
To circle back around, people who come in looking for antidepressants or anti-anxiety medication are doing so because they don’t want to experience depression and anxiety, those negative emotions. The emotions have become intolerable. Now this isn’t me casting judgment. There are cases of profound anxiety and depression where the person looks like they are doing everything in their power to deal with it but are making no headway, but this is not the average case. The average outpatient psychiatry client, derogatorily called “the worried well,” has good and bad days and has done relatively little to work on decreasing these symptoms without medication, let alone has tried to accept these emotions as normal and healthy.
Not only do people want to avoid these negative emotions, but they also want to be happy. That ever-fleeting ephemeral dopamine rush. Is that happiness, or is happiness more tenacious, more long-lasting? Herein lies the problem with the pursuit of happiness. Removing difficult emotions won’t help us accomplish happiness, nor will adding more high octane dopamine activities, be them video games, skydiving, promiscuous sex, or heroin. Happiness can’t be achieved when happiness is the goal. Put that in your pipe and smoke it. We need to seek meaning, fulfillment, purpose. Even in these cases, happiness may never be in our lot. Ideally, once we remove happiness from the end goal, it will be replaced by a more useful, pragmatic ideal.
I'd always read that 85 percent to 90 percent of all depressions would clear up with 6 or 7 weeks of Cognitive Therapy or Cognitive-Behavioral Therapy. And the other 10 to 15 percent was organic. But I certainly find this a very useful perspective. Thank you, Paul.